Presenting finances to patients is what follows after presenting treatment to patients.
Before you do this step, it’s assumed that the doctor, the hygienist, as well as the treatment coordinator have done their part in going over importance of treatment.
If you haven’t seen the video on how to present treatment to patients, you can do so by going to the link posted below this video.
This video is for doctors who present their own finances, for treatment coordinators and other front desk personnel who are responsible for presenting treatment cost and financing to patients.
Instead of focusing on a bunch of theories, I’m going to share exactly how I present to patients.
I’m no guru in presenting finances, I’m just going to show you what’s working in my practice.
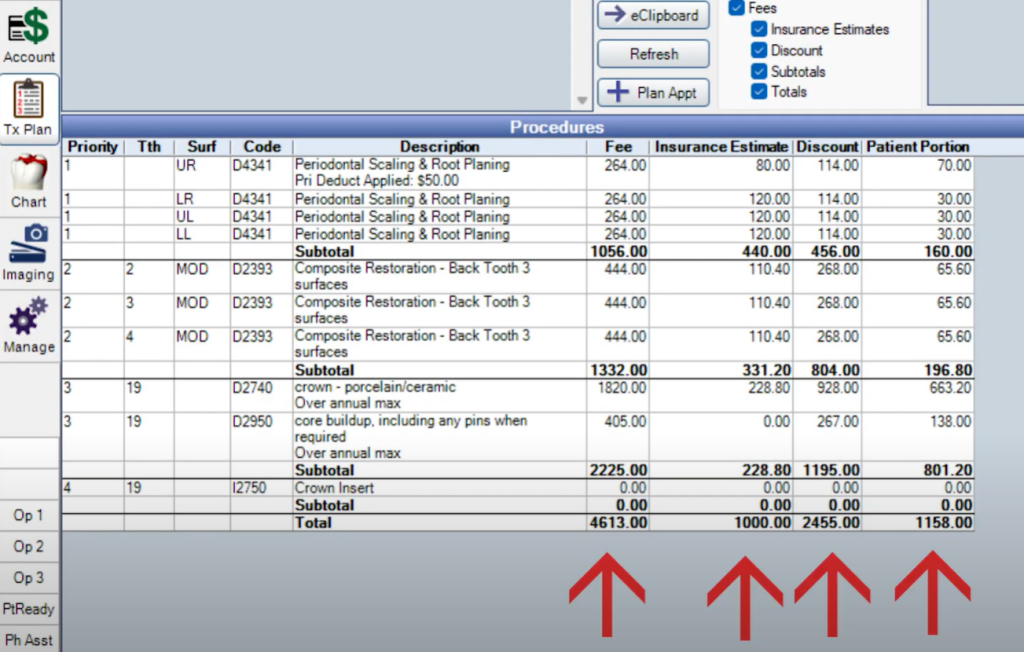
I’m going to start with a small treatment plan where the treatment plan includes full mouth scaling, some restorative, and few crowns.
Remember, you don’t have to be using Open Dental as your practice management system, but you can implement the same concepts for whichever scheduling system you use in your practice.
By the time I’m ready to present finances, there are certain assumptions I’m going to make:
- You and team members have gone over the clinical importance of treatment and risks of not getting work done.
- If the patient has insurance, insurance is already verified and correctly attached to this patient’s chart, so patient’s out of pocket can be calculated correctly.
- It’s important to have the order of the treatment in correct sequence. You’re not trying to plan out the next two years, but at lest the first few visits.
Since I present from the operatory, I make sure the patient is seated up and I’m in front of them.
I point to the screen where I’ve pulled up the treatment plan.
You can also do this on paper – whatever works for you.
At the first glance, the patient has no idea what they’re looking at because
- There are clinical terms they haven’t heard before.
- There are four columns of just fees, so at first glance looks overwhelming.
- They’re going to see some insurance terminology on the treatment plan – for instance, deductible, insurance maxing out, etc..
So, my goal is to divert their attention away from the details and get them to focus only on the big things they care about:
- What’s going to be done at the next visit and what it’s going to cost for them out of pocket
- What total can they expect overall
As I’m pointing to the treatment plan, I’ll mention the clinical jargon on the treatment plan, and also explain in layman’s terms what it is because I’ve already discussed it before I started the financial discussion.
“The composites are your white fillings that we talked about that need to be placed to remove existing decay under the old fillings.”
If there’s a core and crown listed on the treatment plan, I don’t say “well, for your core buildup, your out-of-pocket is this much, and for the crown is this much.”
I quote the total of the core and the crown as one fee – “the cap that we discussed that needs to be placed on upper left area to prevent further fracture and avoid a root canal, your out-of-pocket is going to be so and so.”
So let’s pause here. You’re maybe wondering about insurance downgrading composite fillings to amalgam fillings, and downgrading the ceramic crowns to cast metal crowns.
There are plans that cover composites up to bicuspids and then downgrade for molars.
I NEVER get into these details.
By getting into all the details about the downgrades, it actually confuses the patient even more.
Put yourself in the patient’s shoes. They’re still processing all the information you’ve been telling them for the past few minutes and what it all means.
And now you’re also trying to describe the nuances of insurance details and why they have a different out of pocket from a filling on one tooth to another tooth.
Or what the difference is between the 2 surface filling vs the 3 surface filling.
It doesn’t matter to the patient as much as you think.
You think by giving all the details of the insurance, patient will understand more of how much this is going to cost.
It’s the opposite.
Even after simplifying the treatment plan like I’ve just discussed, patients will still forget what ACTUALLY is the plan for the first visit when they come back.
We always assume a downgrade for composite restorations and crowns, so if the insurance ends up not downgrading, then there’s a credit left on the patient’s account once the claim comes in.
Always remember that it’s better to have credits on patients accounts than balances.
Chasing patients for balance will increase the work for your team – phone follow-ups, sending statements, etc.
Except for rare occasions , statements never need to be sent to patients.
Let’s look at an example of a larger treatment plan:
How do you approach presenting finances to someone who has this large of a treatment plan – where it involves insurance and patient out of pocket is going to be in the range of 5-10K?
I’m going to skip examples of full mouth rehabs like All-on-X and full mouth crowns – because for most of us, it’s not very common.
I’m going to focus on a treatment plan that is mixed with simple restorative, to basic periodontal work, some implants, some root canals, and some crowns.
I’m also going to assume the patient has insurance and they have a typical maximum of let’s say $2500 / year.
When I present finances, I present it in two different ways. I try to get an idea of how motivated the patient is in moving forwards regardless of the insurance dollars remaining on the plan.
If the patient is seeing you in January and their plan is not renewing until next January, and they’ve got a 2500 max – there’s only so much you’re going to be able to do if you ONLY focus on what the insurance will cover.
Here’s my process when I’m looking at a large treatment plan.
Remember, you can change this to what you feel comfortable doing for the patient – how you approach it maybe different for each patient.
Keep your Dental Treatment Plans simple and break them down
Before you come to this point of presenting finances, you’ve already ordered the treatment in terms of priority after discussing with the patient.
Once I’ve decided with the patient on what needs to be focused on first, I arrange the treatment in phases.
So phase 1 will be everything we need to focus on next until the end of the year.
If I do it this way, I have a better idea of how to give the patient the closest estimate of out of pocket responsibility for the whole phase 1.
Why do I break it up?
Let’s assume the patient wants to some treatment this year and leave some for next year.
According to their plan, the insurance is maxing out in the middle of their treatment plan.
So, If I were to give the patient total out-of-pocket for the entire treatment plan – the estimate that I’ll be providing based on what I see in the software will not be even close to accurate.
And what about if something changes in the middle of the treatment plan?
What if the tooth you’re trying to save fractures while the patient is waiting to get it done until next year?
So, by breaking the treatment plan in phases you’re simplifying it for the patient to understand what’s happening.
And you’re making it easy for yourself and your team when you’re presenting finances for this treatment plan.
Focus less on the insurance restrictions and more on risk of not moving forward
If the patient decides to go beyond what their plan will cover for the year, I don’t focus on the fact that insurance is only covering up to $2500 and they’re ending up paying the difference.
While going over the treatment plan with the patient, you may be following each line item on the plan as it’s written on the software.
But, once the insurance is maxed out, and if you’re pointing out the fact that for each line item, they’re now paying more out of pocket, it’s constantly reminding the patient that they’re paying more than they should.
You think you’re helping the patient more by giving these details, but you’re actually overwhelming them, and now they’re hesitant to move forward.
While the patient is looking at the plan, I’ll show the whole total for phase I of their treatment plan.
I’ll then mention the maximum reimbursement we can expect from the insurance is [whatever remaining on the plan] and your out-of-pocket responsibility is so and so.
Then, I remind them of the risks we already discussed during the examination – and say to them:
Having gone over the risk of those teeth that may fracture like we discussed already – and if this looks like it fits your budget for the rest of the year, I’d recommend moving forward asap with the next appointment.
Once we’ve gotten close to the end of phase I, we can again start the discussion of phase II of treatment plan to make sure your insurance reimbursement is maximized and minimize what you pay out of pocket.
By saying it this way, I’m focusing less on the insurance limitations, and instead letting them know how we can work with them to break up the treatment in phases.
Allow for flexibility
We want the patient to move forward with ALL of their treatment ASAP regardless of their insurance limitations.
But in reality, every patient is different.
I can best explain in the diagram below:
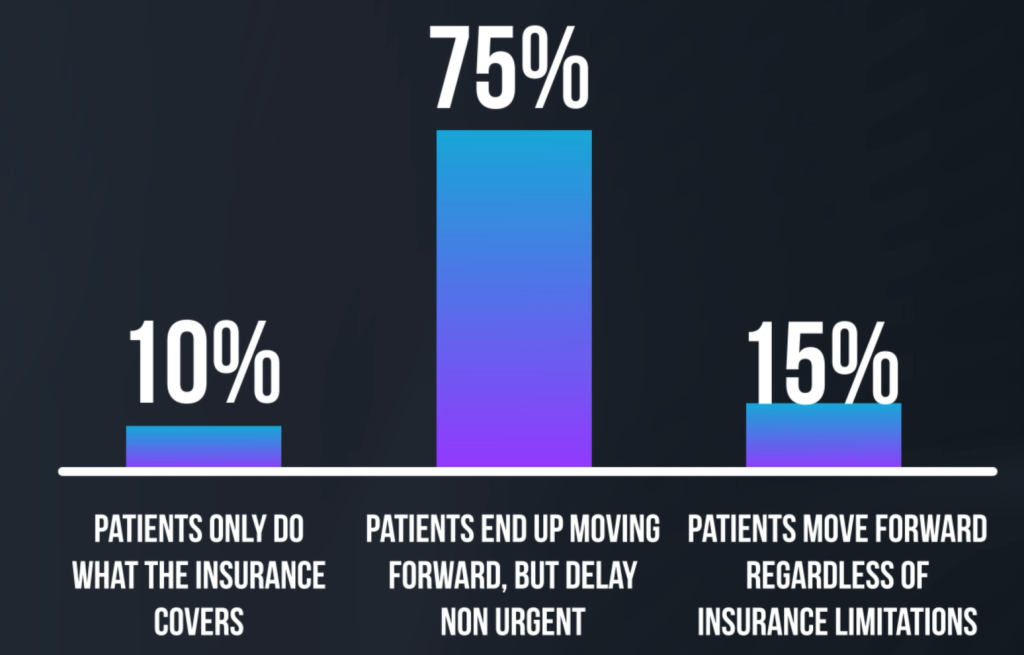
In my practice, 10% of the time when I present financials to patients – they’ll do ONLY what the insurance covers and wait the next eight months until their plan renews to do the next stuff.
75% of patients end up doing both – Once they’ve understood that the teeth at most risk need to be dealt with right away – they’ll move forward with it even though the insurance will max out in middle of treatment.
But, then they’ll wait on certain things until the plan renews, to maximize the insurance reimbursement and minimize their out of pocket.
For instance, once the three out of the four root canals are done this year – they may move forward with getting two crowns this year and the third root canal, I’ll close with a post/core and wait to do the crown on it next year.
And there are those patients, which usually fall into the 15% of all cases – that move forward with everything regardless of insurance limitations.
Don’t rush the financials
If you’re the doctor and you’re presenting finances yourself, you don’t have to finish the entire discussion in one visit.
I don’t always present treatment and discuss financial arrangement for the entire treatment plan the same day,
There are times I split up the time. I summarize what I’ve discussed and break it up into phases.
The only cost I let the patient know during the first visit is what they’ll be responsible for at their NEXT visit, which, if couple days or weeks away, gives me time to put together a customized treatment plan, cost and financial arrangement – like you see in the image below.
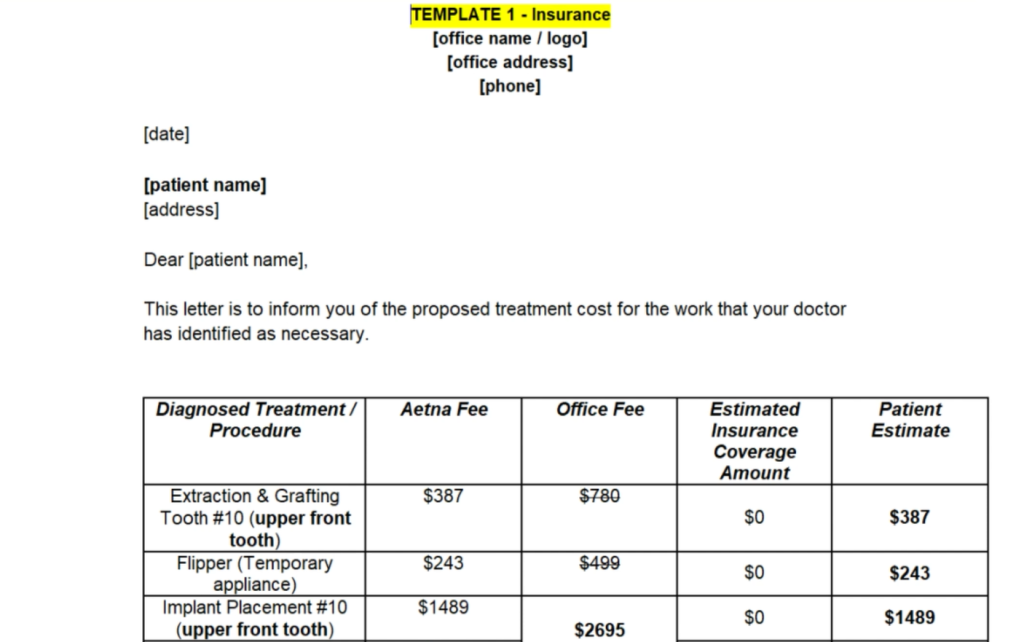
If you haven’t yet seen my video on Financial Arrangement and Treatment planning, I go over in detail how I approach patients who may have larger treatment plans when it involves multiple visits.
Payment Options and Financial Policies
Now that you’ve gone over the cost, it’s time to go over the payment options, talk about your financial policies and have the patient sign any necessary agreement forms.
For Financial policies, I’m referring to things like:
- When does your office collect copays (at time of service or after you’ve sent the claim to the insurance and received payment on it and then billing the patient for the remaining balance)
- What happens when a patient has dual insurance coverage: when do you collect copays if a patient has two insurances?
- What happens when a patient’s insurance becomes inactive in the middle of treatment
You may be offering third party payment plans (like CareCredit), in house financing, prepayment discount, etc.
Whatever it maybe, you should have it all on a simple financial agreement form – and have the patient sign off on how the patient plans on making financial arrangements.
Instead of going into all the details here, I strongly recommend you watch the video on Financial Policy and Agreement Forms – I discuss what payment policies you should have in place to keep the money owed to you at a minimum, best practices when it comes to dual insurances, and details on the payment options you can offer and things you need to watch out for.
Presenting financial policies and payment options is always done at the front by my treatment coordinator. I can present treatment plan and cost, but policies and payment options are discussed at the front.
Scheduling the appointment
Once I’ve gotten to the end of the treatment plan, I’m listening carefully and observing their body language to see how they respond.
Without asking a close ended question that they can usually respond with a simple yes or no, I immediately focus on the next step during the patient visit – which is actually making the appointment for the work the patient needs to come back for.
I turn off the monitor in front of them, , I look at my other monitor at the 12’o clock position and give them two options first to make the next appointment.
If those don’t work, I ask them their schedule, and make the appointment accordingly.
“So depending on your schedule, I have either Tuesday next week, or Thursday afternoon. You tell me what works for you and we’ll get started”
This should be done regardless who’s doing the financial discussion.
If your treatment coordinator is presenting treatment, cost and payment options , they need to make sure there’s an appointment set up for the patient to get started with work.
If for ANY reason, an appointment is not scheduled – ALWAYS ALWAYS get permission to follow-up with the patient to see when you can call them to schedule the appointment.
Always remember, if something isn’t working in your practice, you need to become aware.
But to find out what’s not working, you need to do it enough times and then you’re going to change it over time.
Some quick tips to summarize everything we’ve discussed so far:
- Keep your treatment plans simple – break it up if you have to
- Don’t confuse the patient
- Don’t offer gazillion financial options – offer few that are simple to manage for your team
- Always close your presentation with the patient by scheduling an appointment and if none scheduled – then make sure to set up a reminder to follow-up for treatment!